

BACKGROUND: The Canadian Hemophilia Bleeding Disorders Registry (CBDR) is a clinical database for patients in Canada with bleeding disorders. It was launched on July 1, 2015 and is used by all Canadian Hemophilia Treatment Centers (HTCs) to assist in managing the treatment of hemophilia and other bleeding disorders. CBDR integrates with the patient data entry platform, myCBDR, allowing direct acquisition of infusions, bleeding events, and other patient reported outcome (PRO) data. In August 2018, Emicizumab was approved by Health Canada and made available for the treatment of persons with hemophilia A (PwHA) with inhibitors, and to a small number of PwHA without inhibitors via compassionate access beginning November 2019. With the anticipated change in treatment patterns, disease outcomes, and unique safety consideration (e.g. thrombotic events) with use of Emicizumab, we aim to use CBDR data to describe the current demographics, outcomes, and treatment patterns of hemophilia A patients in Canada before emicizumab. This analysis will provide evidence for and inform on the feasibility and data quality/completeness of the CBDR database to assess the impact of Emicizumab on hemophilia outcomes.
METHODS: De-identified data was extracted from the CBDR database for all registered hemophilia A patients who had not received Emicizumab between January 2018 and December 2019. Data is presented in aggregate as mean ± SD, median [IQR] or frequency (%). Annual bleeding rates (ABR) and annual joint bleeding rates (AJBR) were calculated as (total number of bleeds/ duration of follow-up)*365.25 for each patient with at least one treated bleed. Treatment plans during the 2-year period were defined following a two-step operationalization prioritizing ITI and prophylaxis. Treatment groups are not mutually exclusive as one patient may have used more than one treatment plan over the 2-year study duration. This study received research ethics board approval and abides by the guiding principles of the Declaration of Helsinki.
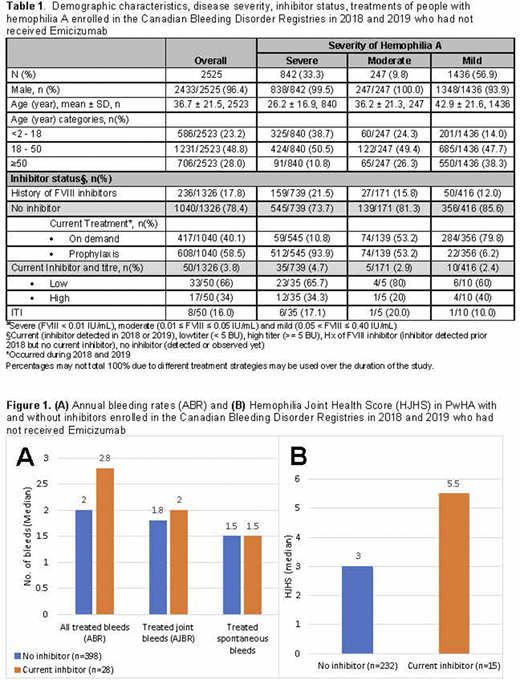
RESULTS: We identified 2525 PwHA registered in CBDR who had not received Emicizumab during the study period. Demographic characteristics, inhibitor status, and treatments are found in Table 1. Mean(±SD) age for the entire cohort was 36.7±21.5 years with 23.2% ≤ 18 years. Inhibitor status was missing in 47.5%. In those with inhibitor status available, 3.8% (50/1326) have FVIII inhibitor present [Low responders 66% (33/50), High responders 34% (17/50)], 17.8% (236/1326) had a history of FVIII inhibitors, and 78.4% (1040/1326) have no current or historical inhibitor. Of the high-responders, 29.4% (5/17) received immune tolerance induction (ITI), 52.9% (9/17) received prophylaxis and 52.9% (9/17) received on demand treatment. Median ABR (IQR) [2.8 (1.5, 4.6) vs. 2.0 (1.0, 5.5), p=0.691] and median AJBR (IQR) [2.0 (0.9, 3.0) vs. 1.8 (1.0, 4.5), p=0.669] are slightly higher in PwHA with inhibitor (n=28) compared to PwHA without inhibitor (n=398) (Figure 1A). Median Hemophilia Joint Health Scores (HJHS) were higher in PwHA with inhibitors (n=15) compared to PwHA without inhibitor (n=232) [5.5 (0.0, 34.0) vs.3.0 (0,16), p=0.781] (Figure 1B). However, the tests werenumbers are not sufficiently powered due to fewer number of observations, highlighting the importance of up-to-date and complete record entry.
CONCLUSION: This analysis confirms the feasibility of using de-identified data extracted from the CBDR database to provide a snapshot of the PwHA demographics, treatments, bleeding, and joint status outcomes over a defined period (i.e. before starting Emicizumab). Incomplete data reporting accounts for missing inhibitor status, so interpretation must be done cautiously and account for data gaps. Encouraging complete and up-to-date data entry will be important for maintaining data quality and accuracy. As more Canadian PwHA switch to Emicizumab, CBDR will allow us to compare treatment patterns and patient outcomes before and after starting Emicizumab. This will inform hemophilia treaters and regulatory authorities of the real-world safety and efficacy outcomes of Emicizumab in PwHA with and without inhibitors.
Lee:Bayer: Honoraria; Takeda: Consultancy, Honoraria, Speakers Bureau. Germini:Bayer: Research Funding; NovoNordisk: Research Funding; Roche: Research Funding; Takeda: Research Funding. Poon:Pfizer: Other: honoraria for advisory board meeting attendance; CSL-Behring: Other: honoraria for advisory board meeting attendance, Research Funding; Bioverative/Sanofi: Other: honoraria for advisory board meeting attendance; Bayer: Other: honoraria for advisory board meeting attendance, Research Funding; Roche: Other: honoraria for advisory board meeting attendance; Novo Nordisk: Other: honoraria for advisory board meeting attendance; Takeda: Other: honoraria for advisory board meeting attendance. Shang:F. Hoffmann-La Roche Ltd: Current Employment, Current equity holder in publicly-traded company, Other: All authors received support for third party writing assistance, furnished by Scott Battle, PhD, provided by F. Hoffmann-La Roche, Basel, Switzerland.. Nissen:F. Hoffmann-La Roche Ltd: Current Employment; GSK: Research Funding; Novartis: Research Funding; Actelion: Consultancy. Meier:F. Hoffmann-La Roche Ltd: Current Employment, Current equity holder in publicly-traded company. Sima:F. Hoffmann-La Roche Ltd/Genentech: Current Employment, Current equity holder in publicly-traded company, Other: All authors received support for third party writing assistance, furnished by Scott Battle, PhD, provided by F. Hoffmann-La Roche, Basel, Switzerland.. Matino:Sobi: Honoraria; Pfizer: Honoraria, Research Funding; Bioverativ: Honoraria; Sigilon: Honoraria. Iorio:Sanofi: Research Funding; Roche: Research Funding; Pfizer: Research Funding; Octapharma: Research Funding; NovoNordisk: Research Funding; BioMarin: Research Funding; Bayer: Research Funding; Spark: Research Funding; Takeda: Research Funding; Uniqure: Research Funding; Freeline: Research Funding; CSL: Research Funding; Grifols: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal